
{kind=link}
Abstract
Introduction: Laparoscopic port-site infections have emerged as an important cause of postoperative morbidity following laparoscopic surgery. The aim of this study was to analyze contemporary data regarding laparoscopic surgery-associated port-site infections and to determine their appropriate treatment modalities.
Methods: This prospective study was conducted in the Department of Surgery at Enam Medical College Hospital during the period from 8 May 2010 to 10 June 2011. A total of 156 patients were selected for the study. Data were analyzed using SPSS version 10 and MS Excel 2016.
Results: A total of 156 patients were included in the study. The majority of patients belonged to the 40–60 years age group, accounting for 86 (55.13%) cases, and most participants were female, comprising 96 (61.54%) patients. The highest number of infections was observed following laparoscopic cholecystectomy, affecting 107 (68.59%) patients. The most isolated organism was Mycobacterium chelonae, identified in 56 (35.90%) cases. In the treatment profile, most patients were successfully treated with clarithromycin, accounting for 44 (28.21%) cases, with a treatment duration of six months or longer.
Conclusion: Port-site infection is a rare but significant complication of laparoscopic surgery. Non-tuberculous mycobacteria are the most common organisms responsible for these infections. Strict adherence to proper cleaning and sterilization protocols for laparoscopic instruments, along with the use of appropriate sterilizing agents, is essential to minimize and prevent this complication.
Key words: post laparoscopic complications, port site infections, laparoscopic surgery.
- Introduction
Laparoscopic techniques have revolutionized the field of surgery over the years. The first laparoscopic surgery, laparoscopic cholecystectomy, was reported by Philips Mouret in 1987, and since then the approach has been widely adopted for numerous surgical procedures, including appendectomy, herniorrhaphy, colonic surgery, gastric surgery, urological surgery, and gynecological surgery1-5. The major advantages of laparoscopic surgery include reduced postoperative pain, quicker recovery and return to normal activities, shorter hospital stay, and fewer postoperative complications. Consequently, it has brought about a paradigm shift in the management of various surgical diseases. However, laparoscopic surgery is also associated with a distinct set of complications, particularly those related to gaining access to the abdominal cavity. Inadvertent bowel injury and major vascular injury, although uncommon, are potentially life-threatening complications that usually occur during the initial access phase 26,27. Among the various complications, port-site infection (PSI) is one of the most important yet largely preventable complications. The reported incidence of PSI varies from 3.3% to 8%, depending on the geographical area and the type of surgery performed 6,7. Port-site infection is a type of surgical-site infection (SSI) that is generally confined to the skin and soft tissues, and rarely the muscles, surrounding the trocar insertion sites through which surgeons gain access to the abdominal cavity. These infections typically present within one month following operative procedure 8. Port-site infections can significantly diminish the advantages of laparoscopic surgery, as patients often become distressed by the persistent and indolent nature of the infection, leading to loss of confidence in the operating surgeon 7. Furthermore, laparoscopic port-site infections contribute substantially to patient morbidity, prolonged hospital stay and increased financial burden 25.
The aim of this study was to determine the morbidity associated with port-site infections following laparoscopic surgery and to suggest an appropriate treatment regimen for their management.
- Objectives
General objective:
- To observe the contemporary data on laparoscopic port site infections.
- To determine the appropriate treatment modalities for port-site infections.
- Methodology & Materials
This prospective study was conducted in the Department of Surgery at Enam Medical College Hospital during the period from 8 May 2010 to 10 June 2011. Patients who were suspected of developing port-site infections following different laparoscopic surgical procedures were included in the study. The clinical features considered for inclusion were delayed wound healing, wound breakdown after initial healing, redness or discharge from the wound, nodules in or around the wound site, and non-responsiveness to empirical antibiotic therapy. A total of 156 cases were selected by random sampling.
The clinical records of these patients were maintained using a predesigned proforma that included demographic details, type of complications, underlying risk factors, treatment modalities, outcomes, and follow-up findings. Data were analyzed using SPSS version 10 and MS Excel 2016. Variables were expressed in terms of frequencies and percentages.
- Result
Among the 156 study patients, the largest proportion belonged to the 40–60-year age group, comprising 86(55.13%) patients, followed by the 20–40-year age group with 42(26.92%) patients and the 60–80-year age group with 28(17.95%) patients [Figure-I]. In terms of sex distribution, there were 60(38.46%) male patients and 96(61.54%) female patients, indicating that females constituted the majority of the study population [Figure-II].
The distribution of laparoscopic port-site infections according to the type of surgery showed that the highest number of infections occurred following laparoscopic cholecystectomy, accounting for 107(68.59%) patients, followed by laparoscopic appendicectomy with 35(22.44%) patients. The fewest infections were observed in cases where the type of laparoscopic surgery was not specified, comprising 14(8.93%) patients. With respect to port-site location, the umbilical port was the most affected. Umbilical infections were reported in 67(42.95%) patients undergoing laparoscopic cholecystectomy, 31(19.87%) patients undergoing laparoscopic appendicectomy, and 14(8.97%) patients in the unspecified laparoscopic surgery group. In laparoscopic cholecystectomy, epigastric port infections occurred in 26(16.67%) patients, lateral port infections in 4(2.56%) patients, suprapubic port infections in 6(3.85%) patients, left iliac port infections in 1(0.64%) patient, and infections at unspecified port sites in 3(1.92%) patients. In laparoscopic appendicectomy, unspecified port-site infections were noted in 4(2.56%) patients [Table-I].
Analysis of the mycobacterial isolates revealed that Mycobacterium chelonae infection was the most frequently identified organism, with 56(35.90%) cases. This was followed by Mycobacterium massiliense infection in 38(24.36%) cases, Tuberculosis in 18(11.54%) cases, and Mycobacterium abscessus infection in 13(8.33%) cases. Unspecified mycobacterial species were reported in 7(4.49%) cases, while Mycobacterium fortuitum infection was identified in 3(1.92%) cases. The least common isolates were Mycobacterium wolinskyi infection and Mycobacterium neoaurum infection, each detected in 1(0.64%) case. In addition, Staphylococcus aureus infection was identified in 14(8.97%) cases among gram-positive organisms, and Pseudomonas infection was identified in 5(3.21%) cases among gram-negative organisms [Table-II].
According to the treatment data, the highest number of patients were successfully treated with Clarithromycin alone, with 44(28.21%) patients receiving therapy for six months or longer. This was followed by Polymyxin B in 28(17.95%) patients for four months, and anti-tubercular therapy in 27(17.31%) patients for less than six months. Combination therapy with Clarithromycin and Ciprofloxacin was used in 22(14.10%) patients for six months or longer. Amikacin combined with Cefoxitin or Imipenem was administered to 18(11.54%) patients for three weeks. Clarithromycin plus Cotrimoxazole was prescribed to 7(4.49%) patients for two weeks. The least commonly used regimens were Clarithromycin plus Doxycycline, administered to 5(3.21%) patients for more than four months, and intravenous Amikacin followed by oral Ofloxacin or Ciprofloxacin for two weeks [Table-III].
Figure-I: Distribute the study patients according to age (N=156)
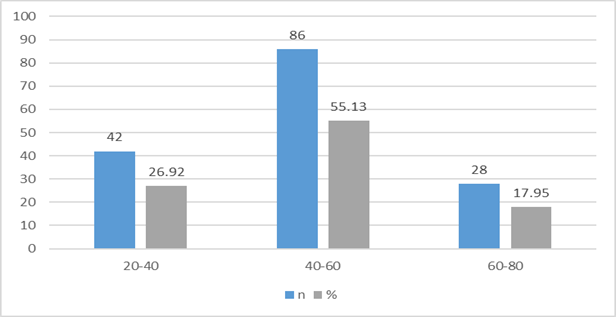
Figure-II: Distribute the study patients according to gender (N=156)
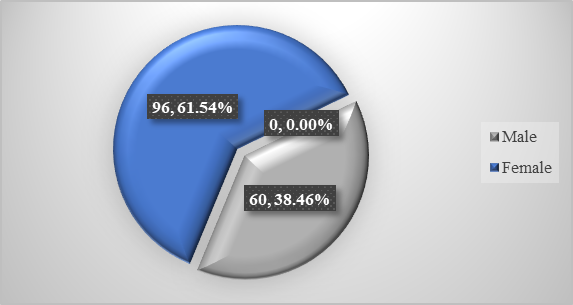
Table-I: Port wise distribution of cases of laparoscopic port site infections (N=156)
| Site of port infections | Laparoscopic cholecystectomy | Laparoscopic appendicectomy | Not specified | |||
| n | % | n | % | n | % | |
| Umbilical | 67 | 42.95 | 31 | 19.87 | 14 | 8.97 |
| Epigastric | 26 | 16.67 | ||||
| Lateral | 4 | 2.56 | ||||
| Suprapubic | 6 | 3.85 | ||||
| Left iliac | 1 | 0.64 | ||||
| Not specified | 3 | 1.92 | 4 | 2.56 | ||
| Number of cases | 107 | 68.59 | 35 | 22.44 | 14 | 8.97 |
Table-II: Distribute the study patients according to the mycobacterial isolates (N=156)
| Micro-organisms | n | % | |
| Mycobacterium | tuberculosis | 18 | 11.54 |
| chelonae | 56 | 35.90 | |
| fortuitum | 3 | 1.92 | |
| abscessus | 13 | 8.33 | |
| wolinskyi | 1 | 0.64 | |
| massiliense | 38 | 24.36 | |
| neoaurum | 1 | 0.64 | |
| Gram positive | Staphylococcus aureus | 14 | 8.97 |
| Gram negative | Pseudomonas | 5 | 3.21 |
| Not specified | 7 | 4.49 | |
Table-III: Distribute the study patients according to the duration of anti-microbial drugs
| Antibiotics | Duration | N | % |
| Anti-tubercular therapy | <6 months | 27 | 17.31 |
| Clarithromycin | ≥6 months | 44 | 28.21 |
| Clarithromycin + Ciprofloxacin | ≥6 months | 22 | 14.10 |
| Clarithromycin + Cotrimoxazole | ≤4 months | 7 | 4.49 |
| Clarithromycin + Doxicycline | >4months | 5 | 3.21 |
| Amikacin (IV), then oral Ofloxacin/Ciprofloxacin | 2 weeks | 5 | 3.21 |
| Amikacin + Cefoxitin/Imipenem | 3 weeks | 18 | 11.54 |
| PB: Polymyxin B | 4 months | 28 | 17.95 |
- Discussion
Among the 156 patients included in the study, the highest proportion belonged to the 40–60-year age group, comprising 86(55.13%) patients, followed by the 20–40-year age group with 42(26.92%) patients and the 60–80-year age group with 28(17.95%) patients. In terms of sex distribution, there were 60(38.46%) male patients and 96(61.54%) female patients, indicating a predominance of female patients. In another study, 492 patients were included, of whom 346 were female and 146 were male. The mean age of the patients was 46.5±21.20 years (Range: 4.5 to 107 years)10.
The present study demonstrated the port-wise distribution of laparoscopic port-site infections. The highest number of infections occurred following laparoscopic cholecystectomy, accounting for 107(68.59%) patients, followed by laparoscopic appendicectomy with 35(22.44%) patients. The lowest number of infections was observed in cases where the type of laparoscopic surgery was not specified, comprising 14(8.93%) patients. With regard to the site of infection, the umbilical port was the most frequently affected. Umbilical infections were reported in 67(42.95%) patients who underwent laparoscopic cholecystectomy, 31(19.87%) patients who underwent laparoscopic appendicectomy, and 14(8.97%) patients in the unspecified laparoscopic surgery group. In laparoscopic cholecystectomy, epigastric port infections occurred in 26(16.67%) patients, lateral port infections in 4(2.56%) patients, suprapubic port infections in 6(3.85%) patients, left iliac port infections in 1(0.64%) patient, and infections at unspecified port sites in 3(1.92%) patients. In laparoscopic appendicectomy, unspecified port-site infections were observed in 4(2.56%) patients 10.
Dense adhesions surrounding the gallbladder can make dissection technically challenging, while a tense and distended gallbladder that has not been decompressed is particularly susceptible to perforation 11,12. Gallbladder perforation commonly occurs during manipulation with laparoscopic instruments or during dissection from the liver bed. Spillage of gallstones may also result from slippage of the cystic duct clip or tearing of the gallbladder during retrieval through the port site 13. Patients with wound infections may present with varying degrees of abdominal pain, with or without signs of peritoneal irritation, as well as nausea, vomiting, or anorexia. In some cases, they may develop empyema or persistent non-healing fistulae 14. Because these symptoms are non-specific, they often mimic other more common conditions and may not be distinguishable based on history and physical examination alone. Abscess formation has been reported to occur as early as 4 days after laparoscopic cholecystectomy and as late as 10 years following surgery15.
Analysis of the mycobacterial isolates showed that Mycobacterium chelonae infection was the most frequently identified organism, accounting for 56(35.90%) cases. This was followed by Mycobacterium massiliense infection in 38(24.36%) cases, Tuberculosis in 18(11.54%) cases, and Mycobacterium abscessus infection in 13(8.33%) cases. Unspecified mycobacterial species were identified in 7(4.49%) cases, while Mycobacterium fortuitum infection was detected in 3(1.92%) cases. The least frequently isolated organisms were Mycobacterium wolinskyi infection and Mycobacterium neoaurum infection, each identified in 1(0.64%) case. In addition, Staphylococcus aureus infection was isolated in 14(8.97%) cases among gram-positive organisms, whereas Pseudomonas infection was identified in 5(3.21%) cases among gram-negative organisms.
In another study conducted in India, 624 cases of port-site infection were evaluated. Microorganisms were identified in 50% of cases, with Mycobacterium chelonae infection accounting for 47% and Mycobacterium massiliense infection accounting for 23.5% of isolates. Overall, 287 infections were caused by Mycobacterium species, of which rapidly growing mycobacteria constituted the majority (91%). Among all mycobacterial isolates, Tuberculosis was identified in 13 cases (5%). Gram-positive and gram-negative organisms were also recognized as causes of port-site infection and were included in the study as part of surgical site infections 9.
Analysis of the treatment outcomes showed that the largest proportion of patients were successfully treated with Clarithromycin alone, with 44(28.21%) patients receiving therapy for six months or longer. This was followed by Polymyxin B in 28(17.95%) patients for four months, anti-tubercular therapy in 27(17.31%) patients for less than six months, and combination therapy with Clarithromycin and Ciprofloxacin in 22(14.10%) patients for six months or longer. A combination of Amikacin and Cefoxitin or Imipenem was administered to 18(11.54%) patients for three weeks, while Clarithromycin plus Cotrimoxazole was used in 7(4.49%) patients for two weeks. The least commonly used regimens were Clarithromycin combined with Doxycycline, administered to 5(3.21%) patients for more than four months, and intravenous Amikacin followed by oral Ofloxacin or Ciprofloxacin for two weeks. Another study reported that combination therapy using Clarithromycin with Doxycycline, Cotrimoxazole, or fluoroquinolones did not produce substantially different outcomes compared with Clarithromycin monotherapy, with both regimens administered for six months. These findings suggest that Clarithromycin for six months may be sufficient for the treatment of port-site infections caused by nontuberculous mycobacteria 9. Several studies have also documented port-site infections caused by Tuberculosis16-19. Another study noted that the management of port-site infections caused by atypical mycobacteria remains controversial, as these organisms often respond poorly to first-line anti-tubercular therapy. Promising results have been reported with second-line anti-tubercular agents, including macrolides such as Clarithromycin, quinolones such as Ciprofloxacin, tetracyclines such as Doxycycline, and aminoglycosides such as Amikacin and Tobramycin, used in various combinations 20-22. Macrolides, particularly Clarithromycin, are the only class of antimicrobials consistently active against Mycobacterium chelonae infection and Mycobacterium abscessus infection 21,23. The Mycobacterium fortuitum infection–chelonae complex has demonstrated resistance to multiple antibiotics due to mutations in porin channels within the bacterial cell wall, which serve as entry sites for antimicrobial agents21. Linezolid has also shown activity against Mycobacterium chelonae infection and has been used successfully as both monotherapy and combination therapy24.
Limitations of the study
As this was not a blinded study, both patient-related and observer-related biases may have influenced the results, particularly in the subjective assessment and recording of outcomes. Consequently, the findings may not fully represent the true clinical scenario.
- Conclusion And Recommendations
Port-site infections are a relatively rare complication of laparoscopic surgery. Among the causative organisms, non-tuberculous mycobacteria are the most frequently implicated pathogens. These organisms generally show susceptibility to agents such as Clarithromycin and Amikacin, while demonstrating resistance to fluoroquinolones and first-line anti-tubercular drugs. In addition to conventional bacterial causes, emerging rapidly growing, multidrug-resistant non-tuberculous mycobacteria represent a growing concern for the surgical community. Strict adherence to proper cleaning protocols and sterilization of laparoscopic instruments using appropriate sterilizing agents is essential to minimize and ideally prevent these complications.
Author of this Article
Dr. Deb Prosad Paul, Professor of Surgery, Enam Medical College, Savar, Dhaka, Bangladesh.
References
- Lei QC, Wang XY, Zheng HZ, Xia XF, Bi JC, Gao XJ, Li N. Laparoscopic Versus Open Colorectal Resection Within Fast Track Programs: An Update Meta-Analysis Based on Randomized Controlled Trials. J Clin Med Res 2015; 7: 594-601 [PMID: 26124904 DOI: 10.14740/jocmr2177w]
- Deng Y, Zhang Y, Guo TK. Laparoscopy-assisted versus open distal gastrectomy for early gastric cancer: A meta-analysis based on seven randomized controlled trials. SurgOncol 2015; 24: 71-77 [PMID: 25791201 DOI: 10.1016/j.suronc.2015.02.003]
- Mehrabi A, Hafezi M, Arvin J, Esmaeilzadeh M, Garoussi C, Emami G, Kössler-Ebs J, Müller-Stich BP, Büchler MW, Hackert T, Diener MK. A systematic review and meta-analysis of laparoscopic versus open distal pancreatectomy for benign and malignant lesions of the pancreas: it’s time to randomize. Surgery 2015; 157: 45-55 [PMID: 25482464 DOI: 10.1016/j.surg.2014.06.081]
- BhaveChittawar P, Franik S, Pouwer AW, Farquhar C. Minimally invasive surgical techniques versus open myomectomy for uterine fibroids. Cochrane Database Syst Rev 2014; 10: CD004638 [PMID: 25331441 DOI: 10.1002/14651858.CD004638.pub3]
- Esposito C, St Peter SD, Escolino M, Juang D, Settimi A, Holcomb GW. Laparoscopic versus open inguinal hernia repair in pediatric patients: a systematic review. J LaparoendoscAdvSurg Tech A 2014; 24: 811-818 [PMID: 25299121 DOI: 10.1089/lap.2014.0194] 6 Zacks SL, Sandler RS, Rutledge R, Brown RS. A population-based cohort.
- Karthik S, Augustine AJ, Shibumon MM, Pai MV. Analysis of laparoscopic port site complications: A descriptive study. J Minim
- Sasmal PK, Mishra TS, Rath S, Meher S, Mohapatra D. Port site infection in laparoscopic surgery: A review of its management. World J Clin Cases 2015;3:864-71.
- Centers for Disease Control and Prevention. The National Healthcare Safety Network (NHSN) Manual: Patient Safety Component. Atlanta, GA: Division of Healthcare Quality Promotion, National Center for Emerging and Zoonotic Infections Diseases. p. 9-6. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf. [Last accessed on 2017 Jan 05].
- Mukherjee R, Sengupta S, Bose S (2018) A Critical Appraisal of Port Site Infections: Meta-Analysis of Existing Contemporary Data. J Surg Transplant Sci 6(1): 1065.
- Muhammad Naeem Taj, Y. I. Z. A., 2012. FREQUENCY AND PREVENTION OF LAPAROSCOPIC PORT SITE INFECTION. J Ayub Med Coll Abbottabad , pp. 1-3.
- Russell RCG, Williams NS, Bulstrode CJK (Eds). Wound infections. Bailey and Love’s Short Practice of Surgery, 24th ed. London: Arnold; 2004. p. 129
- Muhe E. Die erstecolecystektomiedurch das lparoskop. Langenbecks Arch KlinChir 1986;369:804.
- Hackan DJ, Rotstein OD. Host response to laparoscopic surgery: mechanisms and clinical correlates. Can J Surg 1998;41:103–11.
- Mir IS, Ahmad M, Ahad B. Establishing pneumoperitoneum safely for laparoscopic surgeries. JK-Practitioner 2005;12(4):224–6.
- Läuffer JM, Krahenbuhl L, Baer HU, Mettler M, Buchler MW. Clinical manifestations of lost gallstones after laparoscopic cholecystectomy: a case report with review of the literature. SurgLaparoscEndosc 1997;7:103–12.
- Kumar SS, Babu KD, Grace RD, Anapian JC, bhaskar M. A study of port site infections in laparoscopic surgeries IOSR-JDMS. 2015; 14: 20-22.
- Ramesh H, Prakash K, Lekha V, Jacob G, Venugopal A, Venugopal B. Port-site tuberculosis after laparoscopy: report of eight cases. SurgEndosc. 2003; 17: 930-932.10.
- Chaudhuri S, Sarkar D, Mukerji R. Diagnosis and management of atypical mycobacterial infection after laparoscopic surgery. Indian J Surg. 2010; 72: 438-442.11.
- Sharma AK, Sharma R, Sharma S. Port site infection in laparoscopic surgeries. Ind Med Gaz. 2013; 224-229.12.
- Verghese S, Agrawal P, Benjamin S. Mycobacterium chelonae causing chronic wound infection and abdominal incisional hernia. Indian J PatholMicrobiol 2014; 57: 335-337 [PMID: 24943783 DOI: 10.4103/0377-4929.134736]
- Chaudhuri S, Sarkar D, Mukerji R. Diagnosis and management of atypical mycobacterial infection after laparoscopic surgery. Indian J Surg 2010; 72: 438-442 [PMID: 22131651 DOI: 10.1007/ s12262-010-0164-7]
- Wallace RJ, Meier A, Brown BA, Zhang Y, Sander P, Onyi GO, Böttger EC. Genetic basis for clarithromycin resistance among isolates of Mycobacterium chelonae and Mycobacterium abscessus. Antimicrob Agents Chemother 1996; 40: 1676-1681 [PMID: 8807061].
- Svetlíková Z, Skovierová H, Niederweis M, Gaillard JL, McDonnell G, Jackson M. Role of porins in the susceptibility of Mycobacterium smegmatis and Mycobacterium chelonae to aldehyde-based disinfectants and drugs. Antimicrob Agents Chemother 2009; 53: 4015-4018 [PMID: 19581465 DOI: 10.1128/AAC.00590-09.
- Wallace RJ, Brown-Elliott BA, Ward SC, Crist CJ, Mann LB, Wilson RW. Activities of linezolid against rapidly growing mycobacteria. Antimicrob Agents Chemother 2001; 45: 764-767 [PMID: 11181357 DOI: 10.1128/AAC.45.3.764-767.2001]
- Sasmal PK, Mishra TS, Rath S, Meher S, Mohapatra D. Port site infection in laparoscopic surgery: A review of its management. World J Clin Cases 2015; 3(10): 864-871 Available from: URL: http://www.wjgnet.com/2307-8960/full/v3/i10/864.htm DOI: http://dx.doi.org/10.12998/wjcc.v3.i10.864
- Ahmad G, Duffy JM, Phillips K, Watson A. Laparoscopic entry techniques. Cochrane Database Syst Rev 2008;2:CD006583.
- Jansen FW, Kolkman W, Bakkum EA, de Kroon CD, Trimbos-Kemper TC, Trimbos JB. Complications of laparoscopy: An inquiry about closed- versus open-entry technique. Am J ObstetGynecol 2004;190:634-8