{kind=link}
Abstract
Background: Non-Hodgkin’s lymphoma (NHL) with pulmonary involvement is uncommon, and primary pulmonary lymphoma (PPL) is exceedingly rare. Its radiologic appearance often mimics metastatic disease.
Case Presentation: A 50-year-old female presented with anorexia and cervical lymphadenopathy came for evaluation and management. Chest radiograph and CT scan demonstrated multiple bilateral pulmonary nodules without abdominal organ involvement. Core biopsy of a pulmonary lesion confirmed the diagnosis of NHL, B-cell type.
Conclusion: This case underscores the importance of considering NHL in the differential diagnosis of multiple pulmonary nodules and highlights the role of histopathology in establishing a definitive diagnosis.
Keywords: Non-Hodgkin’s lymphoma, pulmonary lymphoma, B-cell lymphoma, pulmonary nodules
Introduction
Non-Hodgkin’s lymphoma (NHL) encompasses a heterogeneous group of lymphoproliferative disorders with variable clinical presentations. Extranodal disease occurs in approximately one-third of cases, most commonly involving the gastrointestinal tract, skin, and central nervous system.1 Pulmonary involvement is rare and is usually secondary to disseminated disease. Primary pulmonary lymphoma (PPL) represents less than 1% of all NHL cases and 0.5% of primary pulmonary malignancies.2
Radiologically, PPL can manifest as single or multiple nodules, masses, or infiltrates, which often mimic pulmonary metastases or infectious diseases.3 Tissue biopsy and immunohistochemistry are essential for accurate diagnosis.
We report a case of pulmonary presentation of NHL, B-cell type, in a middle-aged female with diffuse bilateral nodules and no abdominal involvement.
Case Presentation
A 50-year-old female presented with a several-week history of anorexia. On examination, she was found to have palpable cervical lymphadenopathy. There was no history of fever, chronic cough, hemoptysis, or weight loss.
• Laboratory investigations were unremarkable, with no evidence of organ dysfunction.
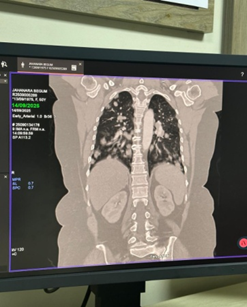
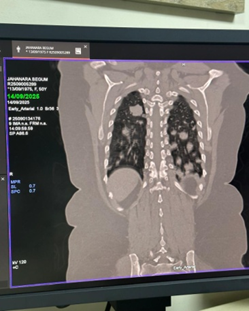
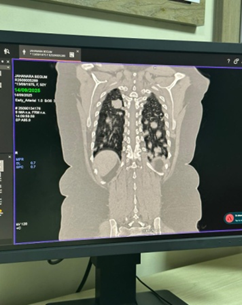
• Chest radiograph revealed multiple nodular opacities in both lung fields.
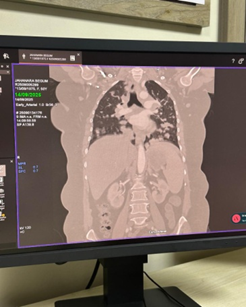
• CT chest demonstrated numerous, variable-sized nodules scattered throughout both lungs, with no mediastinal mass, pleural effusion, or consolidation.
• CT abdomen showed normal hepatosplenic and abdominal organ morphology.
Given the radiological appearance, the differential diagnosis included pulmonary lymphoma versus metastatic disease.
Histopathology: Core biopsy of one pulmonary nodule revealed diffuse infiltration by atypical lymphoid cells. Immunohistochemistry demonstrated positivity for CD20, confirming Non-Hodgkin’s lymphoma, B-cell type.
The patient was referred to the oncology department for staging and initiation of chemotherapy.
Discussion
Pulmonary manifestations of lymphoma are rare, particularly when presenting as multiple bilateral nodules. The primary differential diagnosis in such cases is metastatic disease from an occult primary tumor.4 However, absence of extrapulmonary primary lesions and confirmatory biopsy findings supported the diagnosis of pulmonary NHL in this case.
Clinically, patients may present with nonspecific systemic symptoms such as anorexia, malaise, or B-symptoms (fever, weight loss, night sweats). In our patient, anorexia and cervical lymphadenopathy were the only initial findings.
Radiological patterns of pulmonary lymphoma include:
• Solitary or multiple nodules
• Alveolar consolidation
• Interstitial infiltrates5
This variability often leads to diagnostic delay. Histopathological evaluation, particularly immunohistochemistry, is essential to differentiate NHL from other mimics such as metastatic carcinoma, tuberculosis, or sarcoidosis.
Early diagnosis is critical, as PPL and pulmonary-predominant NHL are potentially treatable with systemic chemotherapy and immunotherapy. Prognosis depends on histological subtype, disease stage, and response to therapy.6
Conclusion
This case highlights that NHL should be considered in the differential diagnosis of multiple pulmonary nodules, especially when abdominal imaging is normal, and no primary malignancy is identified. Histopathological confirmation remains the cornerstone of diagnosis, guiding appropriate management.
Authors of this article
- Prof. Brig. Gen (Retd) Jahangir Alam
MBBS, MCPS, FCPS (Radiology), Fellow MRI (USA),Head – Radiology & Imaging Operation. Square Hospitals LTd.
2. Dr. Shamsun Nahar
MBBS, FCPS, Associate Consultant, Radiology & imaging. Square Hospitals Ltd.
3. Dr. Arunangshu Das
MBBS. FCPS, Consultant, Oncology, Square Hospitals Ltd.
4. Dr. Maliha Mannan Ahmed
MBBS (BMC), MBA (ULAB), Masters in Healthcare Leadership (Brown University, USA) and Level 1 Certification on Precision Nutrition. The Executive Editor of The Coronal.
References
1. Zucca E, Roggero E, Bertoni F, Cavalli F. Primary extranodal non-Hodgkin’s lymphomas. Part 1: Gastrointestinal, cutaneous and genitourinary lymphomas. Ann Oncol. 1997;8(8):727–737.
2. Cadranel J, Wislez M, Antoine M. Primary pulmonary lymphoma. Eur Respir J. 2002;20(3):750–762.
3. Ahmed S, Kussick SJ, Siddiqui AK, Bhuiya TA, Khan A, Sarewitz S, et al. Bronchial-associated lymphoid tissue lymphoma: a clinical study of a rare disease. Eur J Cancer. 2004;40(9):1320–1326.
4. Cordier JF, Chailleux E, Lauque D, Reynaud-Gaubert M, Dietemann-Molard A, Dalphin JC, et al. Primary pulmonary lymphomas. A clinical study of 70 cases in nonimmunocompromised patients. Chest. 1993;103(1):201–208.
5. Koss MN, Hochholzer L, Nichols PW, Wehunt WD, Lazarus AA. Primary non-Hodgkin’s lymphoma and pseudolymphoma of lung: a study of 161 patients. Hum Pathol. 1983;14(12):1024–1038.
6. Ferraro P, Trastek VF, Adlakha H, Deschamps C, Allen MS, Pairolero PC. Primary non-Hodgkin’s lymphoma of the lung. Ann Thorac Surg. 2000;69(4):993–997.