{kind=link}
Introduction
Central venous occlusion is a frequent and serious complication resulting from the repeated and long-term use of high-flow central venous catheters, which are indispensable for procedures like hemodialysis, chemotherapy, and parenteral nutrition. The pathogenesis often involves chronic endothelial injury, leading to intimal hyperplasia and, eventually, total fibrotic occlusion. This condition can severely limit necessary vascular access, particularly for hemodialysis patients who are dependent on functioning access sites for life-sustaining treatment. Loss of central venous access necessitates creative and often complex interventional strategies. The study introduces SNR as a highly specialized, cutting-edge technique designed to restore patency in these long-standing, densely fibrotic, and otherwise impenetrable occluded veins when standard wire-and-catheter techniques have failed. Successful recanalization preserves venous pathways, thus avoiding more invasive surgical options or the need to resort to less optimal or less durable access sites.1
Materials and Methods
A. Patient Population and Enrollment
- Timeframe: January 2012 to December 2014. This two-year period suggests a high-volume interventional setting, even for a rare procedure.
- Inclusion Criteria: Five patients with clinical and venographic evidence of central venous obstruction. The obstruction must have been severe enough to warrant this aggressive intervention, likely after conventional recanalization attempts failed.
- Demographics: Mean age of the intervention group was 28.2 years, which is notably young for a hemodialysis population often facing chronic access issues. 4 out of 5 patients were male. The relatively young age of the cohort may reflect severe, long-term dependence on central access since childhood or early adulthood.2
B. Procedure Details (Sharp Needle Recanalization – SNR)
The core principle of the SNR technique involves simultaneous bi-directional access to overcome the occlusion, establishing coaxial alignment to ensure the needle enters the patent distal lumen. This approach is critical for safety and success in chronic total occlusions (CTOs).
- Access Points: Simultaneous transjugular (upper extremity, representing the pressurized or downstream segment relative to the heart) and transfemoral (lower extremity, typically the upstream, access-only segment) catheterization were utilized to exactly define the extent of the occlusion and create two “targets” for the sharp needle.
- Recanalization Tool: A specialized BRK1 needle was specifically used. This type of needle is commonly employed in transseptal puncture in cardiology, highlighting its design for precise, intentional perforation of tough, fibrotic tissue.
- Guidance: The recanalization was performed under meticulous triangulation fluoroscopy, guiding the sharp needle from the downstream territory (often the femoral side, moving cranially) toward the pressurized upstream territory (the jugular side, moving caudally, or vice-versa depending on the occlusion site). This controlled transgression minimizes the risk of cardiac or mediastinal injury. The two accesses allow for controlled entry and exit points.3
- Steps After Access:
- Establishment of a through-and-through access (connecting the upper and lower venous segments) with a guidewire is the immediate goal, securing the path.
- Subsequent balloon dilatation and stenting (as implied by the discussion and image captions) were performed after successful transgression. Balloon angioplasty opens the newly created channel, and stenting is typically necessary to maintain vessel patency, overcoming the elastic recoil and preventing rapid restenosis typical of chronic central vein lesions.
- Catheter Placement: A Permanent Transjugular tunneled catheter was placed after successful recanalization. This is the final step, providing durable vascular access necessary for ongoing treatment, such as hemodialysis. The choice of the permanent tunneled catheter is crucial for longevity.
C. Outcome Assessment
- Technical Success: Confirmation of reanalyzed vein patency via intra-procedure imaging (e.g., angiography/venography). This is the immediate measure of success the physical creation of a patent lumen.
- Catheter Patency/Function:
- Assessed radiologically at the end of the procedure, ensuring appropriate placement and flow dynamics.
- Adequacy of catheter flow was assessed using the Fresenius 5008 Cordiax hemodialysis machine, providing a real-world functional measure. This is a critical metric, as an open vein is useless if it cannot sustain the high flow rates (typically >300 ml/min) required for efficient dialysis.4
- Complications: Meticulous observation for procedural complications (e.g., vessel perforation, hemorrhage, pneumothorax, nerve injury) and subsequent follow-up complications (e.g., re-occlusion, infection).
III. Results
The study reports high technical success and good functional outcomes in this small cohort, validating the SNR approach for difficult cases.
| Metric | Finding | Details |
| Technical Success Rate | 80% (4 out of 5 cases) | Four out of five cases were successfully recanalized, indicating the complexity of the one failed attempt. |
| Complications | 0% | There were no complications noted during the procedure or subsequent follow-up. This is a crucial finding, supporting the safety profile of the technique when performed by experienced operators. |
| Mean Catheter Flow Rate | 340 ml/min | This flow rate was assessed post-procedure, exceeding the minimum requirements for high-efficiency hemodialysis and confirming functional success. |
| Catheter Placement Site | 3 out of 4 successful catheters were placed in the right jugular vein. | This suggests the right internal jugular vein was the preferred target access for the tunneled catheter post-recanalization. |
Snaring of Wire
Balloon Dilatation
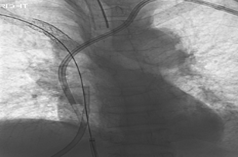
Final Image
Discussion
Technical Rationale
The paper notes that sharp recanalization becomes an indispensable tool when standard catheter and guidewire techniques fail to connect the two patent venous lumina across a chronic, impenetrable occlusion. The fibrosis in chronic lesions makes conventional wire manipulation virtually impossible, necessitating the use of a stiff, sharp instrument like the BRK1 needle to puncture the dense tissue plane.
Indications for SNR
The indications highlight the severity of the patient population for whom SNR is reserved:
- Symptomatic superior vena cava (SVC) syndrome: Caused by central occlusion, leading to debilitating facial and upper extremity swelling.
- Massive upper extremity swelling: Resulting from impaired venous return.
- Dysfunctional dialysis fistulae: Central stenosis often causes high venous pressures that lead to poor flow and failure of peripheral arteriovenous accesses (fistulae or grafts).
- Need for large-bore central venous access: Necessary for high-flow therapies like hemodialysis when other sites are exhausted.5
Comparison and Safety
Based on the small number of patients, the authors tentatively conclude that the success rate for sharp recanalization (80%) does not appear to significantly differ from that of standard catheter-guidewire recanalization for less challenging lesions. This suggests that even for the most difficult lesions, SNR offers comparable efficacy. Crucially, the procedure is deemed safe in this series, with zero reported complications, emphasizing that in expert hands, the high-risk nature of using a sharp instrument can be mitigated by advanced imaging and careful technique.
Conclusion
The procedure is available in many tertiary centers in Riyadh, has an 80% technical success rate, and represents a viable, high-impact option for patients who have experienced multiple access failures and are awaiting renal transplantation. For this challenging patient group, SNR offers a bridge therapy by restoring functional vascular access, significantly improving their quality of life and ensuring continuity of life-saving dialysis treatments while they wait for a permanent solution like a kidney transplant. The study strongly supports the integration of SNR into the armamentarium of complex interventional radiology procedures for vascular access salvage.
Author of this article
Author
AUTHOR NAME-
1.DR. EBADUR RAHMAN, SENIOR CONSULTANT, NEPHROLOGY, EVERCARE HOSPITAL DHAKA,EMAIL-ebadur.rahman@evercarebd.com
CO-AUTHOR-
- DR. RUBAIYA RAHIM
- DR. FAIROOZ RAISA
- Dr. ANZUMAN ARA
- Dr. Ummay Farwa
- Dr. Asma Jalal Panjery
- Dr. A. F M. Abul Foiz MD. Noman
7. DR. REZOYANA NAZIM, SENIOR SPECIALIST, NEPHROLOGY, EVERCARE HOSPITAL DHAKA, EMAIL- dr.esha03@gmail.com
8.DR. AHMED KHALED, SENIOR CONSULTANT, HISTOPATHOLOGY, EVERCARE HOSPITAL DHAKA,EMAIL-ahmed.khaled@evercarebd.com
9.BRIG. GEN.DR. SM MAHBUBUL ALAM, SENIOR CONSULTANT, HISTOPATHOLOGY, EVERCARE HOSPITAL DHAKA,EMAIL-mahbubul.alam@evercarebd.com
10. Dr. Arif Mahmud
11. Zahid Hossain
12. Dr. Sultana Parveen
References
1.Gonsalves CF, Eschelman DJ, Sullivan KL, et al. Incidence of central vein stenosis and occlusion following upper extremity PICC and port placement. Cardiovasc Interv Radiol. 2003;26:123-127.
2. Lumsden AB, MacDonald MJ, Isiklar H, et al. Central venous stenosis in the hemodialysis patient: Incidence and efficacy of endovascular treatment. Cardiovasc Surg. 1997;5:504-509.
3. Altman SD. A practical approach for diagnosis and treatment of central venous stenosis and occlusion. Semin Vasc Surg. 2007;20:189-194.
4. Criado E, Marston WAS, Jaques PF, et al. Proximal venous outflow obstruction in patients with upper extremity arteriovenous dialysis access. Ann Vasc Surg. 1994;8:530-535. 5. Veldtman GR, Hartley A, Visram N, et al. Radiofrequency applications in congenital heart disease. Expert Rev Cardiovasc Ther. 2004;2:117-126