
{kind=link}
Summary:
Fetal hydrocephalus is a congenital condition characterized by a buildup of cerebrospinal fluid (CSF) in the baby’s brain, which increases intracranial pressure and causes potential brain damage. Hydrocephalus pregnancy may be complicated with progression of this condition, breech presentation, preterm delivery, fetal distress and increased need of caesarean birth.it may cause cervical tear, rupture of uterus, injury to rectum and injury to bladder during delivery. Retained fetal head is a rare complication during breech delivery in a hydrocephalus baby. It is associated with increased maternal and fetal morbidity as well as mortality. A 30 years old lady G4P3A3, at 38 weeks with breech presentation, known case of having hydrocephalic baby admitted in to obstetrics & gynae department in CuMCH with labor pain & home trial along with head retention. She was found moderately anaemic, dehydrated and hemodynamically compromised. After resuscitating the patient the dead fetus head was decompressed by craniopuncture and delivered vaginally. During exploration of uterine cavity, uterine rupture was diagnosed and decision was taken for laparotomy. Immediate surgical intervention including failure of repair of the tear followed by total hysterectomy was done to save the life of this patient. Labor complications can be significantly increased by fetal hydrocephalus specially in breech presentation. Routine antenatal care and prompt obstetric management helps to reduce such complications.
Key words: Congenital hydrocephalus, retained fetal head, breech delivery, Rupture uterus.
Introduction:
Congenital hydrocephalus is a condition where ventricular distension occurs due to an increase in cerebrospinal fluid volume. Incidence of this condition ranges from 0.3 to 1 per 1000 births in the world.1 Breech presentation can occur at term around 3-4% of singleton pregnancies which causes significant maternal and fetal risks that includes fetal head entrapment, specially in fetal anomalies such as hydrocephalus. Severe hydrocephalus can complicate both vaginal and cesarean delivery. Prenatal ultrasound is necessary for diagnosing fetal hydrocephalus and a planned delivery favorably cesarean section to minimize the complications.2 This is s case report highlighting the challenges faced during management of a multiparous woman in labor with history of home trial and head entrapment due to fetal hydrocephalus and breech presentation, highlighting the essential role of antenatal care and emergency obstetric procedures.
Case presentation:
A 30 years old multiparous woman G4P3A3, presented at 38 weeks of gestation with history of irregular antenatal care. She had 3 previous normal vaginal delivery. She did ultrasound once at 36 weeks and diagnosed to have a hydrocephalic baby with breech presentation. BPD was 100mm and both lateral ventricles were enlarged right lateral ventricle was 24.8mm and left lateral ventricle was 31mm.3rd ventricle was also dilated. Local doctor referred her to obstetrician but she did not come. At her 38 weeks pregnancy she came with labor pain & home trial along with head entrapment after delivery of the body of baby. Abdominal examination revealed SFH was 28 weeks. There was a hard globular mass felt like fetal head, on vaginal examination dead fetal body was hanging outside the introitus but head was retained. Immediate Resuscitation and investigations were done for the patient. CSF fluid was drained by introducing a 18G spinocaine needle. When the size of head was reduced head was delivered by malar flexion & shoulder traction. Active management of 3rd stage of labour was given. Uterine cavity was explored and a cervical tear on right side which extended up to the fundus of uterus was found. Consent was taken for laparotomy. After that laparotomy was done & ruptured uterus extending to right sided broad ligament was found with significant haematoma. Repairing the uterus but failed, then total hysterectomy was done and 2 unit blood was transfused to minimize the ongoing obstetric haemorrhage. Postoperative recovery was uneventful. Stitches removed after 6th postoperative day and patient was discharged on that day.

Figure-1: Arrest of aftercoming head
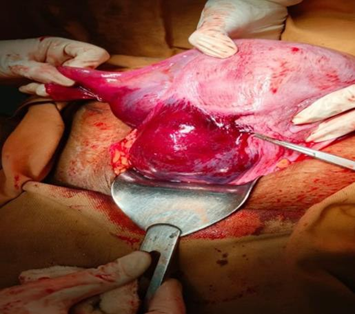
Figure-2: Uterine rupture & Broad ligament hematoma
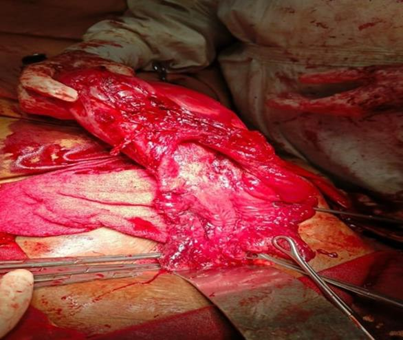
Figure-3: Cervical tear extended up to right sided body of uterus

Figure-4: Repair site after TAH
Discussion:
Congenital Hydrocephalus (CH), an abnormal dilatation of the cerebral ventricles, encompasses a diverse set of disorders present from birth. It causes increased intracranial pressure in the skull and causes enlargement of head, stretching of the sutures and the bones of the head become thin resulting in brain tissue to be compressed and mental defects, in severe cases it can cause death.3 About 3-4% of singleton pregnancies complicated at term by breech presentation and is associated with increased rate of perinatal morbidity and mortality. Cesarean delivery often needed to avoid potential complications like umbilical cord prolapse, birth asphyxia, and traumatic injuries in this population as vaginal delivery in such cases carries increased risks.4 Proper antenatal care with physical examinations and investigations eg. ultrasounds can avoid such an unanticipated obstetric emergency in our case. Fetal anomalies can be identified allowing the case to be managed by multidisciplinary team, proper counseling to patient and delivery planning. In a resource-limited settings, barriers to accessing antenatal care contribute to higher incidences of undiagnosed fetal conditions, underscoring the need for improved healthcare infrastructure and education.5,6
Fetal hydrocephalus, complicates both vaginal and cesarean deliveries due to the increased circumference of fetal head. During breech deliveries, the head may become entrapped, leading to prolonged or obstructed labor and potential fetal hypoxia. Early detection through prenatal imaging is crucial and a well-planned mode of delivery is crucial for reducing associated risks.7 Hydrocephalus is simple to treat if diagnosed early. On the contrary, if not detected early it can be detrimental causing severe injury to mother and baby including fetal head retention, fetal demise and breech presentation,uterine rupture during delivery. In case of hydrocephalus, incomplete rupture can occur even in pregnancy. The importance of ultrasound monitoring is crucial until delivery. Hence, an ultrasound examination is important for exclusion of pelvic disproportion along with the fetal head, so that the fetal head does not harm the mother’s uterus. Therefore, an ultrasound examination must be carried out to ensure that there is no pelvic disproportion with the fetal head, and that the fetal head does not injured the mother’s uterus.8 The management of the after-coming head in breech deliveries is a challenge especially in hydrocephalus. Different maneuvers, such as the Mauriceau-Smellie-Veit and Bracht techniques, may not be effective in cases of significant fetal hydrocephalus. The decision of emergency cesarean section is obligatory. However, timely decision-making and the availability of surgical expertise are the keys of success.9
The whole team should be meticulously ready to combat all the potential maternal complications. It has got pivotal role to proper maternal evaluation during perioperative period to minimize the fatal outcomes. All measures should be taken to limit intra-operative blood loss , as if it occur may be combined with pre-existing nutritional deficiencies, can lead to significant morbidity. Prompt identification and management, including blood transfusion and postoperative monitoring, are vital for optimal maternal outcomes.10,11
Conclusion:
We can recognize the importance of adequate antenatal care on maternal and fetal outcomes with this case. Diagnosis of fetal hydrocephalus, breech presentation should be done with appropriate examinations and routine investigations. Which facilitates the obstetrician to
manage such complex cases with Multidisciplinary team, planned delivery and avoiding complications. Additionally, emergency obstetric team should have sufficient skills and drills with enough equipments to deal with critical situations like fetal head retention. For mother’s recovery process adequate support should be given. Improved healthcare infrastructure and education of community people are needed to overcome the undiagnosed fetal complications in a resource-limited setting.
Authors of this Article
- Prof. Dr. Sartaj Begum, Head, Department of Obstetrics & Gynaecology, Comilla Medical College
- Dr. Sanzida Sharmin, Assistant Professor, Obstetrics & Gynaecology, Kamringarchar, Health Complex, Dhaka
- Dr. Nishat Jahan, Medical Officer, Obstetrics & Gynaecology, Comilla Medical College Hospital
References:
- Van Landingham, M., T. V Nguyen, A. Roberts, A. D. Parent, and J. Zhang. 2009. ―Risk Factors of Congenital Hydrocephalus: A 10 Year Retrospective Study.‖ Journal of Neurology, Neurosurgery, and Psychiatry 80(2):213–17. doi: 10.1136/jnnp.2008.148932.
- Leblanc F, Khobzaoui M, Cailliau E, et al. Breech presentation induction compared to cephalic presentation: Effectiveness and characteristics. Eur J Obstet Gynecol Reprod Biol. 2023;282:155-60. DOI: https://doi.org/10.1016/j.ejogrb.2020.03.033.
- Alluhaybi, Abdulelah A., Khalid Altuhaini, and Maqsood Ahmad. 2022. ―Fetal Ventriculomegaly: A Review of Literature.‖ Cureus 14(2):18–21. doi:10.7759/cureus.22352.
- Sananès N. Breech Presentation: CNGOF Guidelines for clinical practice-benefits and risks for the neonate and child of planned vaginal delivery versus elective cesarean section. Gynecol Obstet Fertil Senol. 2019;48(1):95-108. DOI:https://doi.org/10.1016/j.gofs.2019.10.023
- Ducarme G. Breech presentation: CNGOF guidelines for clinical practice-external cephalic version and other interventions to turn breech babies to cephalic presentation. Gynecol Obstet Fertil Senol. 2020;48(1) 81-94.DOI: https://doi.org/10.1016/j.gofs.2019.10.024
- Macharey G, Gissler M, Toijonen A, et al. Congenital anomalies in breech presentation: A nationwide record linkage study. Congenital Anomalies. 2021;61(4):112-7. DOI: https://doi.org/10.1111/cga.12411.
- Macharey G, Gissler M, Rahkonen L, et al. Breech presentation at term and associated obstetric risks factors—a nationwide population based cohort study. Arch Gynecol Obstet. 2017;295:833-8. DOI: 10.1007/s00404-016-4283-7.
- Raboel, P. H., J. Jr Bartek, M. Andresen, B. M. Bellander, and B. Romner. 2012. ―Intracranial Pressure Monitoring: Invasive versus Non-Invasive Methods-A Review.‖ Critical Care Research and Practice 2012:950393. doi: 10.1155/2012/950393.
- Mostello D, Chang JJ, Bai F, et al. Breech presentation at delivery: a marker for congenital anomaly?. J Perinatol. 2014;34(1):11-5. DOI: https://doi.org/10.1038/jp.2013.1328.
- Hamza A, Herr D, Solomayer EF, et al. Polyhydramnios: causes, diagnosis and therapy. Geburtshilfe und Frauenheilkunde. 2013;73(12):1241-6. DOI: https://doi.org/10.1055/S-0033- 1360163.
- Macharey G, Gissler M, Rahkonen L, et al. Breech presentation at term and associated obstetric risks factors- a nationwide population based cohort study. Arch Gynecol Obstet. 2017;295:833-8. DOI: 10.1007/s0040