
{kind=link}
Abstract
Stroke is a big health problem in Bangladesh. It causes death and long-term disability. Many patients cannot stay in the hospital for a long time because it costs too much money. We wanted to see if care at home works as well as care in a hospital. We looked at 112 patients who had a stroke. We split them into two groups. One group did exercises at home with help from their family. The other group came to the hospital for therapy. We checked them for 12 weeks using a scale called the Modified Barthel Index (MBI). Both groups got much better by the end. There was no big difference in improvement between the home group and the hospital group. This means home care is a good choice for people who cannot afford the hospital.
Introduction
A stroke happens when blood flow to the brain stops. It happens fast and can last more than 24 hours or cause death. It is the third main cause of death in Bangladesh. Many people who survive a stroke are left with disabilities. They need rehabilitation to get better. Rehabilitation helps them learn to do things again, like walking or dressing.1
In Bangladesh, we do not have enough resources for everyone. Most patients go back to their villages after the initial treatment. They usually go home with disabilities and do not recover fully. The people taking care of them at home often do not know how to help properly.2
Staying in the hospital for therapy is expensive. Many people leave early because they run out of money. Also, it is hard for poor people or old people to travel to the hospital every day. We thought that home-based care could be a good answer. If we teach the family how to help, the patient might get better in their own house.3
We did this study to compare two things. We compared how well patients recover at home versus how well they recover in the hospital. We hope this helps us treat more people in our country.4
Methodology
Study Design and Place
We did this study at the Shaheed Suhrawardy Medical College and Hospital in Dhaka. It was a quasi-experimental study. We did this over six months.
The Patients
We picked patients who had their first stroke within the last 4 weeks. They had to be stable and awake. We did not include patients who were unconscious or had other bad heart or lung problems. In total, we had 112 patients.
The Groups
We divided the patients into two groups:
- Group A (Home Care): These patients could not come to the hospital often. We taught their family caregivers how to do the exercises. The caregivers learned things like how to position the patient in bed and how to help them move. They did this at home.
- Group B (Hospital Care): These patients could come to the hospital. They got therapy from a physiotherapist 5 days a week.
The Treatment
Both groups did similar exercises. We gave them medicine as needed. The exercises depended on how strong their muscles were.
- If they could not move at all, we did passive movements.
- If they could move a little, we helped them stretch and balance.
- We also taught them about bowel and bladder control and deep breathing.
Measurements
We measured their progress using the Modified Barthel Index (MBI). This scale looks at 10 activities like feeding, bathing, dressing, and walking. We checked their score at the start, at 6 weeks, and at 12 weeks.
Results
We looked at the data from 112 patients. Group A had 58 people and Group B had 54 people37.
Table 1: Patient Information
| Information | Home Care (n=58) | Hospital Care (n=54) | P Value |
| Average Age (years) | 55.4 ± 12.8 | 57.9 ± 14.0 | 0.481 |
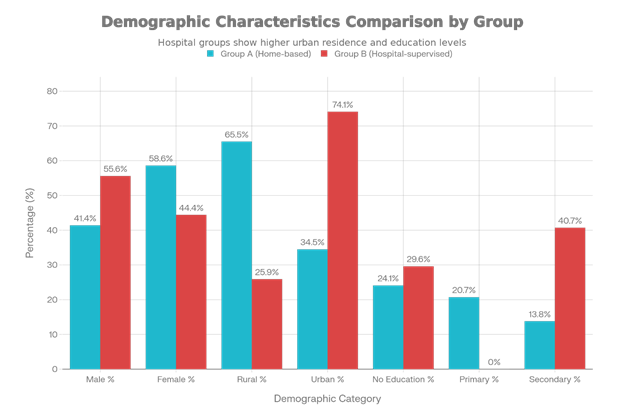
| Male (%) | 41.4 | 55.6 | 0.134 |
| From Village (%) | 65.5 | 25.9 | <0.001 |
| Average Monthly Money | 20,724 TK | 27,074 TK | <0.001 |
Table 2: Health Problems
| Problem | Home Care | Hospital Care | P Value |
| Diabetes (%) | 72.4 | 81.5 | 0.256 |
| High Blood Pressure (%) | 86.2 | 85.2 | 0.877 |
| High Cholesterol (%) | 62.1 | 75.9 | 0.114 |
| Smoking (%) | 44.8 | 59.3 | 0.127 |
Table 3: Improvement Scores
| Time | Home Care | Hospital Care | P Value |
| Start | 5.7 ± 3.5 | 6.9 ± 3.4 | 0.200 |
| 6 Weeks | 8.5 ± 3.9 | 10.1 ± 4.1 | 0.163 |
| 12 Weeks | 11.7 ± 3.7 | 13.1 ± 4.0 | 0.187 |
Comparing the Two Groups
We compared Group A and Group B. We found no big statistical difference between them at any time. The people at home got better just like the people in the hospital.
Discussion
Stroke can make it hard to move or think. We found that home-based care works as well as hospital care. This is good news. Other studies have found similar things.5
In our study, the hospital group had richer people who lived in the city. The people from villages preferred home care because traveling is hard for them. Since this was not a random choice for everyone, the richer people picked the hospital more often.6
Home care has some big benefits. The patient does not have to travel. This stops them from getting anxious about leaving the house. Also, the family gets involved. They learn how to help their loved one. This is very important in a country like Bangladesh where hospital beds are limited.7
A study by Roderick et al. also showed that home care and hospital care have similar results. Another study suggested that long-term results might even be better at home.8
There were some limitations. We did not pick the groups randomly. The patients chose what they could afford or manage. Also, we only did this in one hospital. But the results are still very promising.9
Conclusion
Both home-based care and supervised hospital care help stroke patients get better. The functional improvement is about the same for both. Home-based rehabilitation is feasible and acceptable. It is a very effective alternative for people who cannot afford expensive hospital stays or who live far away.10 We should train more caregivers. Hospitals should have teams to teach families what to do. This can save money and help more people recover from strokes.
Author of this Article
Dr. Mohammad Al-Amin Munshi, MBBS, FCPS, Consultant (Physical Medicine and Rehabilitation). Ortho, CRP, Mirpur, Dhaka.
References
- Truelsen T, Begg S, Mathers C. The global burden of cerebrovascular disease. Geneva: World Health Organization; 2000.
- American Heart Association. Heart Disease & Stroke Statistical Update Fact Sheet Global Burden of Disease. 2020.
- Islam MN, Moniruzzaman M, Khalil MI, Basri R, Alam MK, Loo KW, et al. Burden of stroke in Bangladesh. International journal of stroke. 2013;8(3):211-3.
- Goldstein LB, Adams R, Alberts MJ, Appel LJ, Brass LM, Bushnell CD, et al. Primary prevention of ischemic stroke. Stroke. 2006; 37(6): 1583-633.
- Lopez-Liria R, Vega-Ramírez FA, Rocamora-Perez P, Aguilar-Parra JM, Padilla Gongora D. Comparison of two post-stroke rehabilitation programs: a follow-up study among primary versus specialized health care. PloS one. 2016 Nov 11;11(11):e0166242.
- Rahman MS, Salek AK. Training of caregiver for home care management of stroke survivor at low resource setting. Bangabandhu Sheikh Mujib Medical University Journal. 2016;9(4):193-5.
- Chakraborty PK, Islam MJ, Hossain MS, Barua SK, Rahman S. Profile of Patients Receiving Stroke Rehabilitation in a Tertiary Care Hospital. Chattagram Maa-O-Shishu Hospital Medical College Journal, 2018;17(1):9-12.
- Roderick P, Low J, Day R, Peasgood T, Mullee MA, Turnbull JC, Villar T, Raftery J. Stroke rehabilitation after hospital discharge: a randomized trial comparing domiciliary and day‐hospital care. Age and Ageing. 2001;30(4):303-10.
- Anderson C, Rubenach S, Mhurchu CN, Clark M, Spencer C, Winsor A. Home or hospital for stroke rehabilitation? results of a randomized controlled trial: I: health outcomes at 6 months. Stroke. 2000 May;31(5):1024-31.
- Gladman J, Forster A, Young J. Hospital-and home-based rehabilitation after discharge from hospital for stroke patients: analysis of two trials. Age and ageing. 1995 Jan 1;24(1):49-53.