{kind=link}
ABSTRACT
Introduction and background:
The treatment of completely displaced midshaft clavicle fractures is still controversial, but surgical treatment provides a shorter recovery period and higher union rates than non operative treatment. We sought to compare patient-oriented outcome complication rates following non operative treatment and those after plate fixation of displaced midshaft clavicular fractures.
Methods:
This observational study involving a total of 200 patients was carried out at the Department of Orthopaedic and Traumatology, Chittagong Medical College Hospital, Private hospital, Chattogram, Bangladesh, from 2018 to 2022. Of these, 100 patients who underwent plate fixation were put in Group A, and 100 patients treated non operatively were in Group B. Each patient was followed up for a total of 1 year.
Result:
Among the group A patients, post–operative infection was 3%, and nonunion 2%. Among the group B patients, 10% were malunion, 5% were nonunion, and 5% were delayed unions. The mean time of union in Group A was 6.8 weeks, which was significantly shorter than Group B at 9.4 weeks.
Conclusion:
Operative fixation of a displaced fracture of the clavicular shaft results in improved functional outcome and a lower rate of malunion and nonunion compared with nonoperative treatment at one year of follow-up.
Keywords: Triangular sling, figure of eight bandage, single plate fixation.
INTRODUCTION
Clavicle fractures are a common type of fracture, accounting for 2.6% of all fractures and 5% of adult fracture1 Among clavicle fractures, middle-third fractures make up nearly 82% of cases.2 This is largely due to the unique structure of the clavicle, which is thinnest at the junction of the outer and middle thirds and lacks additional protection from muscles and ligaments.2,3 While there are several treatment options for clavicle fractures, the majority are traditionally treated non-operatively. However, due to its location, a clavicle fracture is often displaced, making non-surgical treatment challenging. Clavicle fractures can occur in people of all ages, but they are more common in children and young adults due to their active lifestyles.4,5 In adolescents, clavicle injuries are often caused by falls from height or participation in sports.5 A significant portion of fractures is also caused by high-energy injuries such as car accidents. There is a bimodal distribution of adult clavicle fractures, with a higher incidence in males under 30 years of age due to high-energy trauma and a second peak in the elderly population due to osteoporosis, which are typically associated with low-energy falls.6 Young adults tend to fracture the mid-shaft of the clavicle, while the elderly are more likely to fracture the lateral end.6 Displaced mid-shaft clavicular fractures, which occur in the middle part of the collarbone, can be treated with plate fixation, a surgical procedure in which a metal plate is attached to the bone using screws to hold it in place during healing. Some studies have suggested that plate fixation may lead to better functional outcomes, such as improved range of motion and strength, compared to non-operative treatment, which involves using a sling or other immobilization device to hold the bone in place while it heals. In the past, non-surgical treatment was preferred for mid-shaft clavicle fractures, even in cases of obvious displacement, due to a low rate of non-union.7,8 However, recent research has found that the nonunion rate of displaced fractures after non-surgical treatment is higher than previously reported. 9,10 There is currently a consensus on non-surgical treatment for mid-shaft clavicle fractures without displacement, but the optimal treatment for displaced mid-shaft clavicle fractures remains controversial. 11The goal of any clavicle fracture treatment method is to achieve bony union while minimizing dysfunction, morbidity, and cosmetic deformity. In non-operative treatment methods, the first step is always shoulder immobilization. This is typically achieved using a simple sling or a figure-of-eight brace. However, there is no clear indication of how long immobilization should be continued, as it can vary depending on the patient’s age and fracture details.11 After immobilization, the physician needs to reposition the fractured bone to its normal location, which becomes more difficult with more compound and displaced fractures. While the movement is generally discouraged, some physicians may recommend starting isometric physiotherapy and resistance exercises after 4-8 weeks of immobilization, depending on residual pain and discomfort. Non-operative treatment can be time-consuming, with complete union often taking 5-7 months. There are several surgical treatment options for clavicle fractures, including inter fragmentary screw fixation, intramedullary (IM) fixation, cerclage wiring, and plate fixation.12 The present study aims to evaluate the functional outcomes of plate fixation for the treatment of displaced mid-shaft clavicle fractures. Plate fixation is a type of internal fixation in which a plate made of surgical-grade stainless steel or titanium is attached to the fractured bone with screws. The plates may be removed in a subsequent surgical procedure. Plate fixation has been shown to significantly reduce the nonunion rate for various types of fractures.13 Plate fixation provides immediate rigid fixation, including rotational stability, which is favorable for early rehabilitation protocols and is technically less demanding. Plate fixation may be an effective treatment for displaced mid-shaft clavicle fractures because it allows the bone to heal in a more anatomically correct position, potentially improving the patient’s range of motion and strength. However, it is important to note that plate fixation is a major surgical procedure with risks and potential complications, including infection, nerve or blood vessel damage, and failure of the plate or screws. This study aims to determine whether the benefits of plate fixation for displaced mid-shaft clavicle fractures outweigh the risks compared to non-operative treatment methods.
OBJECTIVE
General Objective
- To observe the functional outcome of displaced mid-shaft clavicular fracture after plate fixation against the non-operative treatment method
Specific Objectives
- To observe the non-union and malunion rate of plate fixation of the displaced mid-shaft clavicular fractures
MATERILS AND METHODS
This observational study was conducted at the Department of Orthopedic and Traumatology, Chittagong Medical College Hospital & Private Hospitals, Chattogram, Bangladesh. The study duration was 4 years, from July 2018 to June 2022. During this period, data was collected from a total of 200 follow-up interviews who had their displaced midshaft clavicular fracture treated previously. A purposive selection method was used to select the 200-sample size, among which 100 who had been treated with plate fixation were put into Group A, while another hundred who had been treated non-operatively were put into Group B. Data was collected from their final follow-up interview which was conducted 1 year after initial treatment. Informed consent was obtained from each of the participants regarding their participation in the study, and ethical approval was obtained from the ethical review committee of the study hospital.
RESULTS
Table I: Distribution of participants by demographic factors
| Demographic Factors | Group A | Group B | ||
| n | % | n | % | |
| Gender | ||||
| Male | 84 | 84.0% | 81 | 81.0% |
| Female | 16 | 16.0% | 19 | 19.0% |
| Mode of Injury | ||||
| Road traffic accident | 67 | 67.0% | 63 | 63.0% |
| Fall from height | 23 | 23.0% | 23 | 23.0% |
| High-intensity sports | 10 | 10.0% | 14 | 14.0% |
| Side Affected | ||||
| Right | 43 | 43.0% | 40 | 40.0% |
| Left | 57 | 57.0% | 60 | 60.0% |
Among the participants, the overall male prevalence was observed, with 84% male in Group A and 8% male in Group B. Mode of injury was road traffic injury for 67% of Group A and 63% of Group B participants, fall from height for 23% of Group A and 23% of Group B participants, and high-intensity sports for 10% of Group A and 14% of Group B participants. Among the participants of both groups, the left side was more affected, at 57% of Group A and 60% of Group B,
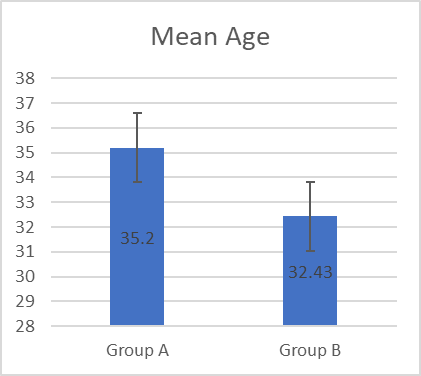
Figure I: Distribution of participants by mean age among groups
The mean age of Group A participants was 35.2 years, while the mean age was 32.43 years for group B
Table II: Distribution of participants by post-operative complications
| Post-Operative Complications | Group A | Group B | P Value | ||
| n | % | n | % | ||
| Post-Operative Infections | 3 | 3.0% | 0 | 0.0% | <0.01 |
| Non-Union | 2 | 2.0% | 5 | 5.0% | |
| Malunion | 0 | 0.0% | 10 | 10.0% | |
| Delayed Union | 0 | 0.0% | 5 | 5.0% | |
| Total | 5 | 5.0% | 20 | 20.0% | |
Among the participants of Group A, a total of 5% had complications, while in Group B, it was 20%. Among Group A participants, 3% had post-operative infections, while 2% had non-union. Among the participants of Group B, 5% had non-union, 10% had malunion, and another 5% had delayed union. The difference in complications between the two groups was statistically significant
Table III: Distribution of participants by time to union
| Time To Union | Group A | Group B | P Value | ||
| n | % | n | % | ||
| <6 weeks | 37 | 37.0% | 0 | 0.0% | <0.01 |
| 6-7 weeks | 32 | 32.0% | 12 | 12.0% | |
| 7-8 weeks | 14 | 14.0% | 15 | 15.0% | |
| 8-10 weeks | 11 | 11.0% | 63 | 61.0% | |
| >10 weeks | 4 | 4.0% | 5 | 24.0% | |
| Non-Union | 2 | 2.0% | 5 | 5.0% | |
| Mean weeks | 6.8 | 9.4 | |||
Among Group A participants, 28% had union within 6 weeks of operation, 42% had union within 6-7 weeks of operation, 15% between 7-8 weeks, 11% between 8-10 weeks, and 4% took over 10 weeks for the union. Among the Group B participants, only 6% had union within 6-7 weeks, 9% had union within 7-8 weeks, 61% had union within 8-10 weeks, and 24% required over 10 weeks to reunion.
Table IV: Distribution of participants by Functional Outcome grading
| Functional Outcome | Group A | Group B | ||
| n | % | n | % | |
| Excellent | 88 | 88.0% | 71 | 71.0% |
| Good | 9 | 9.0% | 18 | 18.0% |
| Poor | 3 | 3.0% | 11 | 11.0% |
Among the patients of Group A, 88% had excellent functional outcomes, 9% had good outcomes and only 3% had a poor outcomes. Among the Group B participants, 71% had excellent functional outcomes, 18% had good functional outcomes, and 11% had poor functional outcome levels.
DISCUSSION
Recent studies have shown an increased tendency of treating clavicle fractures with surgery. The present study was conducted with the final follow-up data of 200 patients, 100 of whom had been treated with the surgical plate fixation method (Group-A), while another 100 had been treated non-operatively (Group B). Male: Female ratio was similar among the participants, with higher male prevalence among both groups. This high incidence of male participants among the displaced mishit clavicular fractures was also observed in other related studies.14 This high male prevalence can be explained by the outgoing nature of the male population, especially in the younger age, putting them at an increased risk of various types of injuries. A reflection of this understanding can be observed in the mode of injury distribution, where a large portion of both groups had suffered from road traffic accidents. Road traffic incident is an extremely common cause of injury, not only for clavicle fractures but also for other orthopedic fractures and complications, as observed from other studies.15 The follow-up interviews of the participants revealed a significant difference in terms of postoperative complications and time to union of bone among the groups.16 Among the present study participants, a total of 5% of the Group-A participants had postoperative complications, while this percentage was 20% among those treated non-operatively. Non-union was observed in only 2 participants of the plate fixation group, and 3% had post-operative infections. On the other hand, among that treated non-operatively, 5% had non-union, another 5% had delayed union and 10% had a malunion. This stark difference in post-operative groups was also observed in other studies as well. 16,17 Infection after surgery is not uncommon and has been observed in a slightly higher or lower percentage among other studies regarding the treatment of clavicle fractures as well.17 In general, the infection rate after a plate fixation for a clavicle fracture can have an incidence rate of 0.4%-7.8%, and our study had a low infection rate.18 Among the non-operative group participants, malunion had the highest prevalence in terms of complications. The mean union duration was 6.8 weeks for those of Group-A, while group-B participants had a mean bone union time of 9.4 weeks. This is another factor where surgical fixation has clear benefits over non-surgical fixation.20 The higher non-union rate among the non-operative participants was also supported by the findings of other clinical trials and meta-analyses, where the non-union rate was often higher compared to our studies.21,22 From the final follow-up data, it can be observed that functional outcome was relatively better among group.23,24 A participants, as 88% had excellent and 9% had good outcomes, compared to 71% excellent and 18% good outcomes among the group B participants.25,26 Poor functional outcome level was observed in 3% of the Group-A participants, which was significantly lower compared to the 11% of Group-B participants.27 This was also supported by the findings of other studies.
LIMITATIONS OF THE STUDY
The study was conducted in a single hospital with a small sample size. So, the results may not represent the whole community.
CONCLUSION
The Operative fixation of a displaced fracture of the clavicular shaft results in improved functional outcome and a lower rate of mal union and nonunion compared with non operative treatment at one year of follow-up.
RECOMENDATION
- As present study was done on a relatively small sample, a large-scale study to be conducted to make the findings of the study generalized to reference population.
- This procedure has wide spectrum of potential complications, which needs continuous evaluation to further improve treatment results.
ACKNOWLEDGEMENT
- We are thankful to the head of the Department Orthopedic & Traumatology and the Director, Chittagong Medical College & Hospital, and the managing Director of Private Hospitals.
DISCOSURE
- All the authors declared no competing interest.
Authors of this Article
Principal Author: Dr.Mahmudur Rahman, Assistant Professor, Department of Orthopedics and Traumatology, Chittagong Medical College, Chattogram, Bangladesh,
Co-Authors:
- Dr. Mohammad Abdul Hye, Assistant professor, Department of Orthopedics and Traumatology, Chittagong Medical College, Chattogram, Bangladesh,
- Dr. Khaled Ibney Anwar, Junior Consultant, Department of Orthopedics and Traumatology, Chittagong Medical College, Chattogram, Bangladesh,
- Dr Heba Hoque, Consultant, Chevron Eye Hospital & research Center, Chattogram
REFERENCES
- Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of clavicle fractures. Journal of shoulder and elbow surgery. 2002 Sep 1;11(5):452-6.
- Jeray KJ. Acute midshaft clavicular fracture. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2007 Apr 1;15(4):239-48.
- Shapira S, Givon U, Pritsch M. Middle third clavicle fractures–diagnosis, complications and treatment. Harefuah. 2011 Sep 1;150(9):725-8.
- Caird MS. Clavicle shaft fractures: are children little adults?. Journal of Pediatric Orthopaedics. 2012 Jun 1;32:S1-4.
- Pecci M, Kreher JB. Clavicle fractures. American family physician. 2008 Jan 1;77(1):65-70.
- Moverley R, Little N, Gulihar A, Singh B. Current concepts in the management of clavicle fractures. Journal of clinical orthopaedics and trauma. 2020 Feb 1;11:S25-30.
- CHARLES S NEER II. 5 Fractures of the distal third of the clavicle. Clinical Orthopaedics and Related Research (1976-2007). 1968 May 1;58:43-50.
- Rowe CR. 4 An Atlas of Anatomy and Treatment of Midclavicular Fractures. Clinical Orthopaedics and Related Research (1976-2007). 1968 May 1;58:29-42.
- Hill JM, McGuire MH, Crosby LA. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. The Journal of bone and joint surgery. British volume. 1997 Jul;79(4):537-8.
- Murray IR, Foster CJ, Eros A, Robinson CM. Risk factors for nonunion after nonoperative treatment of displaced midshaft fractures of the clavicle. JBJS. 2013 Jul 3;95(13):1153-8.
- Van der Meijden OA, Gaskill TR, Millett PJ. Treatment of clavicle fractures: current concepts review. Journal of shoulder and elbow surgery. 2012 Mar 1;21(3):423-9.
- Waldmann S, Benninger E, Meier C. Nonoperative treatment of midshaft clavicle fractures in adults. The open orthopaedics journal. 2018;12:1.
- Lenza M, Faloppa F. Surgical interventions for treating acute fractures or non‐union of the middle third of the clavicle. Cochrane Database of Systematic Reviews. 2015(5).
- Robinson CM, Goudie EB, Murray IR, Jenkins PJ, Ahktar MA, Read EO, Foster CJ, Clark K, Brooksbank AJ, Arthur A, Crowther MA. Open reduction and plate fixation versus nonoperative treatment for displaced midshaft clavicular fractures: a multicenter, randomized, controlled trial. JBJS. 2013 Sep 4;95(17):1576-84.
- Society CO. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial.
- Song HS, Kim H. Current concepts in the treatment of midshaft clavicle fractures in adults. Clinics in Shoulder and Elbow. 2021 Sep;24(3):189.
- Internal Fixation: Plates [Internet]. International Center for Limb Lengthening. 2018 [cited 2022 Dec 8]. Available from: https://www.limblength.org/treatments/lengthening-deformity-correction-devices/internal-fixation-plates/
- Huang X, Xiao H, Xue F. Clavicle nonunion and plate breakage after locking compression plate fixation of displaced midshaft clavicular fractures. Experimental and Therapeutic Medicine. 2020 Jan 1;19(1):308-12.
- Kihlström C, Möller M, Lönn K, Wolf O. Clavicle fractures: epidemiology, classification and treatment of 2 422 fractures in the Swedish Fracture Register; an observational study. BMC musculoskeletal disorders. 2017 Dec;18(1):1-9.
- Tsai SW, Ma HH, Hsu FW, Chou TF, Chen KH, Chiang CC, Chen WM. Risk factors for refracture after plate removal for midshaft clavicle fracture after bone union. Journal of Orthopaedic Surgery and Research. 2019 Dec;14(1):1-8.
- Kulshrestha V, Roy T, Audige L. Operative versus nonoperative management of displaced midshaft clavicle fractures: a prospective cohort study. Journal of orthopaedic trauma. 2011 Jan 1;25(1):31-8.
- McKee RC, Whelan DB, Schemitsch EH, McKee MD. Operative versus nonoperative care of displaced midshaft clavicular fractures: a meta-analysis of randomized clinical trials. JBJS. 2012 Apr 18;94(8):675-84.
- Altamimi SA, McKee MD. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures: Surgical technique. JBJS. 2008 Mar 1;90(Supplement_2_Part_1):1-8.
- Duncan SF, Sperling JW, Steinmann S. Infection after clavicle fractures. Clinical Orthopaedics and Related Research (1976-2007). 2005 Oct 1;439:74-8.
- Wijdicks FJ, Van der Meijden OA, Millett PJ, Verleisdonk EJ, Houwert RM. Systematic review of the complications of plate fixation of clavicle fractures. Archives of orthopaedic and trauma surgery. 2012 May;132(5):617-25.
- Liu PC, Hsieh CH, Chen JC, Lu CC, Chuo CY, Chien SH. Infection after surgical reconstruction of a clavicle fracture using a reconstruction plate: a report of seven cases. The Kaohsiung journal of medical sciences. 2008 Jan;24(1):45-9.