
{kind=link}
ABSTRACT
Background: Status epilepticus (SE) represents the most frequent pediatric neurological emergency, demanding rapid clinical intervention to mitigate long-term sequelae. This study aimed to identify the etiological profile and specific risk factors associated with SE in a cohort of children admitted to a tertiary care facility in Bangladesh.
Methods: A cross-sectional study was conducted at the Department of Pediatrics, Institute of Child and Mother Health (ICMH), Dhaka, between July 2021 and June 2022. A total of 115 children (aged 1 month to <18 years) meeting the clinical criteria for SE (seizure duration ≥5 minutes) were enrolled. Clinical examinations, biochemical assays, cerebrospinal fluid (CSF) analysis, electroencephalography (EEG), and neuro-imaging were utilized for diagnostic evaluation. Data were analyzed using SPSS version 24.0.
Results: The mean age was 4.26 ± 2.90 years, with a male predominance (53.9%). Generalized seizures were the most prevalent type (90.4%). Acute symptomatic etiologies accounted for 70.4% of cases, with febrile convulsions (41.7%) and meningitis (22.6%) being the primary contributors. Febrile convulsions were significantly associated with younger age (mean 2.5 years, p=0.001), whereas meningitis (mean 5.9 years, p=0.001) and epilepsy (mean 5.3 years, p=0.049) were more prevalent in older children. Furthermore, unknown etiology was a significant risk factor for refractory status epilepticus (RSE), accounting for 23.5% of RSE cases (p=0.003).
Conclusion: Febrile convulsions are the leading risk factor for SE in younger children and are typically non-refractory. In contrast, meningitis and pre-existing epilepsy are more frequent in older cohorts. Identification of acute symptomatic causes and unknown etiologies is critical, as they significantly increase the risk of progression to refractory states.
Keywords: Febrile convulsion, epilepsy, Status Epilepticus, meningitis.
INTRODUCTION
Status epilepticus (SE) is a critical neurological emergency characterized by prolonged seizure activity, carrying substantial risk for life-threatening complications and permanent neurological morbidity.1 The global incidence of SE is estimated at 18–28 per 100,000 individuals annually, with a disproportionately high incidence in infants.2 In Bangladesh, the prevalence of SE among children has been reported at 8.2%, with an associated mortality rate of 2.6% for those under the age of 10.3, 4.
The clinical trajectory of SE is influenced by patient age, seizure type, duration, and underlying etiology.5 While SE is classified into generalized, focal, non-convulsive, and neonatal types, Generalized Tonic-Clonic (GTC) seizures are the most common and are associated with the highest rates of morbidity. Common acute triggers include atypical febrile seizures and neuro-infections such as meningitis and encephalitis. 1, 2 In patients with a prior diagnosis of epilepsy, status may be precipitated by sleep deprivation or poor adherence to anti-seizure medications (ASM), formerly referred to as antiepileptic drugs (AEDs). 6
As seizure activity exceeding five minutes significantly increases the risk of pharmaco-resistance and permanent brain injury, rapid identification of risk factors is essential.2, 7 This study aims to delineate these risk factors within a tertiary care setting in Bangladesh to optimize management protocols and reduce associated morbidity.
METHODOLOGY
Study Design and Setting This cross-sectional study was conducted at the Department of Paediatrics, Institute of Child and Mother Health (ICMH), Dhaka, from July 2021 to June 2022.
Inclusion and Ethical Protocols The study enrolled 115 children, aged 1 month to less than 18 years, diagnosed with SE. SE was clinically defined as active seizure activity lasting ≥5 minutes or recurrent seizures without the recovery of consciousness between episodes. Ethical clearance was granted by the Institutional Review Board (IRB) of ICMH, and informed written consent was obtained from the legal guardians of all participants.
Data Collection Following the stabilization of the patient’s airway, breathing, and circulation (ABC), a comprehensive clinical history and neurological examination were performed. Diagnostic investigations included complete blood counts (CBC), random blood sugar, serum calcium, and serum sodium levels. Lumbar puncture for CSF study was performed in suspected cases. EEG was conducted in both awake and sleep states, interpreted by a pediatric neurologist. Neuro-imaging (CT or MRI) was utilized when indicated. SE cases were classified as non-refractory, refractory (RSE), or super refractory status epilepticus (SRSE).
Statistical Analysis Data were processed using SPSS version 24.0. Continuous variables were expressed as mean ± standard deviation (SD), and categorical variables were presented as frequencies and percentages. Associations between variables were assessed using Chi-square tests and unpaired t-tests, with significance defined as p < 0.05.
RESULTS
Demographic Profile The study population (n=115) had a mean age of 4.26 ± 2.90 years, with the 4–6-year age group being the most frequent (35.7%). A slight male predominance was observed (n=62; 53.9%). A family history of febrile seizures was present in 15.7% of cases, while a family history of epilepsy was noted in 13.9%.
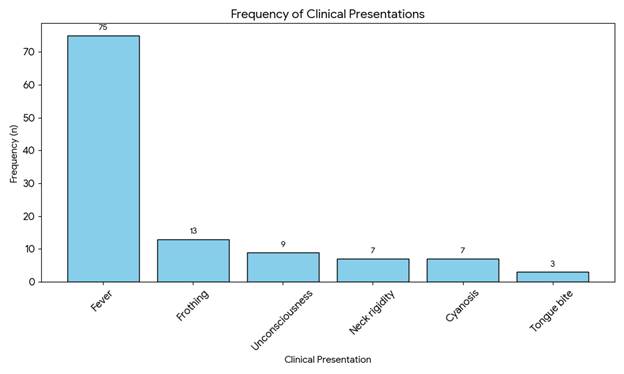
Clinical Presentation Fever was the most common clinical sign at admission, occurring in 65.2% of the children.
| Clinical Presentation | Frequency (n) | Percentage (%) |
| Fever | 75 | 65.2 |
| Frothing | 13 | 11.3 |
| Unconsciousness | 9 | 7.8 |
| Neck rigidity | 7 | 6.1 |
| Cyanosis | 7 | 6.1 |
| Tongue bite | 3 | 2.6 |
Seizure Classification Generalized seizures occurred in 90.4% of patients (n=104), while focal seizures were seen in 9.6% (n=11). Regarding severity, 70.4% were classified as non-refractory, 23.5% as refractory (RSE), and 6.1% as super refractory (SRSE).
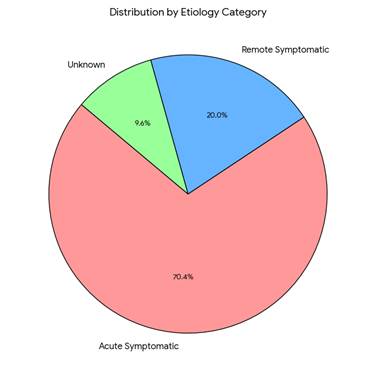
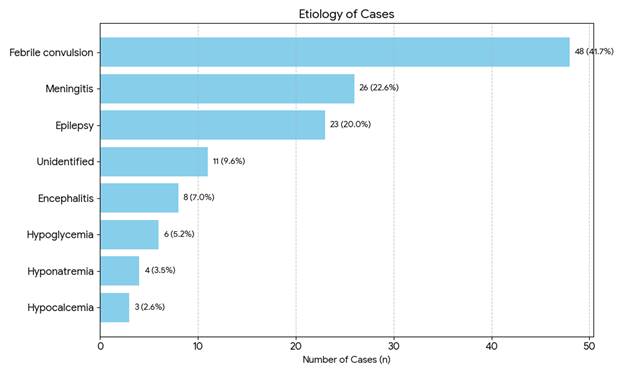
Etiological Findings Acute symptomatic etiologies were the most frequent, identified in 70.4% of cases.
| Etiology Category | Specific Etiology | No. of Cases (n) | Percentage (%) |
| Acute Symptomatic | 81 | 70.4 | |
| Febrile convulsion | 48 | 41.7 | |
| Meningitis | 26 | 22.6 | |
| Encephalitis | 8 | 7.0 | |
| Hypoglycemia | 6 | 5.2 | |
| Hyponatremia | 4 | 3.5 | |
| Hypocalcemia | 3 | 2.6 | |
| Remote Symptomatic | Epilepsy | 23 | 20.0 |
| Unknown | Unidentified | 11 | 9.6 |
Biochemical and Diagnostic Results Metabolic disturbances were infrequent: hypoglycemia (5.2%), hyponatremia (3.5%), and hypocalcemia (2.6%). Among children with a history of epilepsy (n=25), 92% had abnormal EEG findings, most commonly focal epileptogenic areas (39.1%). Neuro-imaging (n=9) was abnormal in 55.6% of those tested, with encephalitis being the most common finding. CSF analysis (n=82) revealed abnormalities in 31.7% of cases; notably, however, none of the cultures yielded positive bacterial growth.
Statistical Associations
- Age-Related Risk Factors: Febrile convulsions were significantly associated with younger age (mean 2.5 years vs. 5.6 years; p=0.001). Conversely, neuro-infections (meningitis, mean 5.9 years; p=0.001) and epilepsy (mean 5.3 years; p=0.049) were significantly associated with older age groups.
- Seizure Duration and ASM Requirement: There was a significant correlation (p=0.001) between seizure duration and the number of ASMs required. Of patients presenting within 30 minutes, 59% were controlled with a single agent—typically Benzodiazepines (BDZ). Conversely, 45.5% of those with seizures exceeding 60 minutes required three agents (BDZ + Phenytoin + Phenobarbitone), and 21.2% required a fourth agent (Midazolam).
- Etiology and Refractoriness: Febrile convulsions were exclusively associated with non-refractory SE (p=0.001). Risk factors significantly associated with RSE included encephalitis (p=0.001), meningitis (p=0.003), and unknown/unidentified etiology (p=0.002). Notably, 23.5% of the refractory cases were of unknown origin compared to only 3.7% in the non-refractory group (p=0.003).
DISCUSSION
The demographic findings of this study a mean age of 4.26 years and a male predominance are consistent with previous regional and international literature. 8,9, 10, 11 The prevalence of generalized seizures (90.4%) also aligns with findings by Alyoubi et al. and Absar et al. 9, 11
A notable finding was the 31.7% CSF abnormality rate, which is higher than the 10.0% to 15.8% reported in studies by Arun et al. and Dasgupta et al.10, 14 From a clinical perspective, the fact that all CSF cultures were negative despite abnormal cell counts and chemistry suggests a high prevalence of viral etiologies or perhaps partially treated bacterial meningitis prior to hospital arrival. This high rate of CSF abnormality may also reflect a more severe clinical presentation in this specific tertiary cohort.
The study identified acute symptomatic etiologies as the primary driver of SE, with neuro-infections (meningitis and encephalitis) significantly predisposing patients to RSE. In contrast, febrile convulsions were highly associated with non-refractory SE, likely explaining why this study observed a lower rate of RSE compared to specialized pediatric intensive care studies like those by Beegum et al. or Kantanen et al. 12, 16
A critical clinical observation was the correlation between seizure duration and the complexity of pharmacotherapy. Prolonged seizures (>60 minutes) necessitated the use of multiple ASMs, including Benzodiazepines, Phenytoin, Phenobarbitone, and Midazolam, reinforcing the necessity of rapid intervention to prevent the transition into pharmaco-resistant states. Furthermore, “unknown etiology” emerged as a significant risk factor for RSE, highlighting the need for more advanced diagnostic tools in treatment-resistant cases.
CONCLUSION & RECOMMENDATIONS
This study demonstrates that febrile convulsions are the most common risk factor for status epilepticus in younger children and are generally responsive to initial ASM therapy. In older children, meningitis and epilepsy are the predominant risk factors. Neuro-infections and unknown etiologies are significant predictors for the development of refractory status epilepticus.
Limitations: The findings are limited by a single-center design and a relatively small sample size, which may impact the generalizability of the data.
Recommendations: Future multicenter studies with larger, randomized cohorts are recommended to validate these risk factors and inform national management guidelines for pediatric status epilepticus.
Author of this Article
Dr. Md Azizul Islam, Emergency Medical Officer, 250 Bed General Hospital, Moulvibazar, Bangladesh.
REFERENCES
- Vafaee-Shahi, M., Soltanieh, E., Saidi, H. & Riahi, A., 2020. Etiology, Risk Factors, Mortality and Morbidity of Status Epilepticus in Children: A Retrospective Cross-Sectional Study in Tehran, Iran. The Open Neurology Journal, 14(1), 95–102.
- Selvan, T., Nagaraj, M.V., Saravanan, P. and Tudu, M.N., 2017. A study of the etiology and short-term outcome of status epilepticus in children. International Journal of Contemporary Pediatrics, 4(3), 878.
- Mohammad, Q.D., Saha, N.C., Alam, M.B., Hoque, S.A., Islam, A., Chowdhury, R.N., et al., 2020. Prevalence of epilepsy in Bangladesh: Results from a national household survey. Epilepsia Open, 5(4), 526–36.
- Chegondi, M., Garland, M.M., Sendi, P., Jayakar, A.R. & Totapally, B.R., 2019. Course and Outcome of Children with Convulsive Status Epilepticus Admitted to a Pediatric Intensive Care Unit. Cureus, 11(4), 1–9.
- Pujar, S. & Scott, R.C., 2019. Long-term outcomes after childhood convulsive status epilepticus. Current Opinion in Pediatrics, 31(6), 763–768.
- Ascoli, M., Ferlazzo, E., Gasparini, S., Mastroianni, G., Citraro, R., Roberti, R., et al., 2021. Epidemiology and outcomes of status epilepticus. International Journal of General Medicine, 14(June), 2965–973.
- Lagae, L., 2020. Paediatric status epilepticus: finally, some evidence-based treatment guidance, but still a long way to go. The Lancet Child and Adolescent Health, 4(5), 351–352.
- Santhanam, I., Yoganathan, S., Sivakumar, V.A., Ramakrishnamurugan, R., Sathish, S. and Thandavarayan, M., 2017. Predictors of outcome in children with status epilepticus during resuscitation in pediatric emergency department: a retrospective observational study. Annals of Indian Academy of Neurology, 20(2), 142–148.
- Alyoubi, R.A., Aljaafari, D.T., Basheikh, M.A., Al- Yahyawi, N.Y., Bakry, M.A., Benhli, N.M., et al., 2021. The etiology and risk factors of convulsive status epilepticus in pediatric patients of tertiary center in saudi arabia. Neurosciences, 26(1), 26–30.
- Arun Prakash, T., TK, S., Rajakumar, P.S. and Shuba, S., 2017. Profile on status epilepticus, clinical features and lab parameters and outcome in pediatric intensive care. International Journal of Contemporary Pediatrics, 4(4), 1310.
- Absar, N., Bhuiyan, S.I., Faruque, F.A. & Talha, A., 2020. Clinical Profile of Febrile Seizure in Children: A Study in a Tertiary Care Hospital, Dhaka, Bangladesh. Scholars Journal of Applied Medical Sciences, 8(11), 2672–676.
- Beegum, M.B., Devakumar, V.K. & Sugunan, S., 2021. Clinico-Etiological Profile and Outcome of Children with Status Epilepticus Admitted in Pediatric Intensive Care Unit of a Tertiary Care Hospital – A Prospective Observational Study. International Journal of Research and Review, 8(7), 473–480.
- Shinnar, S., Pellock, J.M., Berg, A.T., O’Dell, C., Driscoll, S.M., Maytal, J., Moshe, S.L. and DeLorenzo, R.J., 2001. Short-term outcomes of children with febrile status epilepticus. Epilepsia, 42(1), 47-53.
- Dasgupta, S., Guha, S. & Mukherjee, A., 2019. A Study on Etiological Evaluation of Children Aged 2 Months-12 Years with status epilepticus Admitted in a Tertiary Care Centre. Journal of Evolution of Medical and Dental Sciences, 8(32), 2549–553.
- Doumbia, A.K., Koné, O., Dembélé, G., Dembelé, A., Coulibaly, O., Diall, H.G., et al., 2021. Seizures in Children under Five in a Pediatric Ward: Prevalence, Associated Factors and Outcomes. Open Journal of Pediatrics, 11(04), 627–35.
- Kantanen, A.M., Sairanen, J. & Kälviäinen, R., 2019. Incidence of the different stages of status epilepticus in Eastern Finland: A population-based study. Epilepsy and Behavior, 101(1), 1-5.